A stent is a endovascular, cylindrical,
mesh-like, but dilatable structure (by ballon-tipped catheter
or tube), which is inserted into various atherosclerotic arteries,
especially coronary ones, to maintain patency of the vessel
(see figure 95a, 95b)
after having been dilated by inflating the ballon catheter.
Usually the diseased artery has been
dilated to remove the blockage with an angioplasty balloon,
which has been introduced percutaneously with a tube or catheter
inserted into the right femoral artery and guided to the concerned
diseased artery site.
After
the stent is inserted, it is left in place to maintain the opening
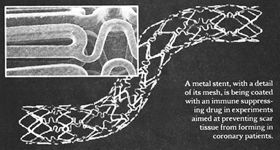
in the previously blocked artery. But in 25% of cases scar tissue
(intimal proliferation) forms as a reaction to the injury from
the dilatation and reblocks the arterial lumen. Recently there
are reports that this reaction can be prevented by coating the
stent with an immunosuppressive drug (a cell-cycle inhibitor)
called rapamycin (sirolimus), previously used to prevent cell
growth and transplant kidney rejection (figure 95c, 95d, 95e).
Reference:Sousa,J.E.
and OthersLack of NeointimalProliferation After Implanation
of Sirolimus-Coated in Stents in Human Coronary Arteries,Circulation,Vol.103,No.2,Jan.16,2001,pp192-195.
Radiation therapy to the stent area is also
being used to prevent this scarring but there is concern that
the radiation may lead to subsequent sarcomas in the coronary
artery or myocardium, coronary arterial aneurysms, or early
rethrombosis. Beta Irradiation is given by positioning a catheter
equipped with a yttrium-90 source at the site dilated by the
ballon and was shown to be effective in reducing the incidence
of restenosis at six months.
(Verin,V.and
Others, Endoluminal Beta-Radiation Therapy for the Preveention
of Coronary Restenosis after Ballon Angioplasty,New England
Journal of Medicince,Jan.25,2001, V.344,N.4,PP.241-242).
Also, Gamma-radiation using a an indwelling
intracoronary ribbon containing a sealed source of iridium-192
has been shown to reduce the rate of restenosis, but was associated
with a higher rate of late thrombosis and increased risk of
myocardial infarction.
(Leon,M.B.
and Others, Localized Intracoronary Gamma-RadiationTherapy To
Inhibit The Recurrence Of Restenosis After Stenting, New England
Journal of Medicince,Jan.25,2001, V.344,N.4,PP250-256).
As measured one year after the procedure,coronary
stenting for multivessel disease is less expensive than bypass
surgery and offers the same degree of protection against death,
stroke, and myocardial infarction. However, stenting is associated
with a greater need for repeated revascularization.
Reference:Serruys,P.T.,and
others,Comparison of Coronary-Artery Bypass Surgery And Stenting
For The Treatment Of Multivessel Disease,N Engl J Med,Vol.344,No.15,April12,2001,1117-1124.
Journal of the American College of Cardiology
Vol. 40, No. 6, 2002
2002 by the American College of Cardiology Foundation ISSN 0735-1097/02/522.00
Published by Elsevier Science Inc. P11 50735-1097(02)02123-X
STATE-OF-THE-ART PAPER
Selection of Coronary Stents
Antonio Colombo, MD, FACC,* Goran
Stankovic, MD,* Jeffrey W. Moses, MD, FACC
Milan, Italy; and New York, New York
In clinical practice, the operator
must decide which stent is most appropriate for the patient.
This article focuses on the features of stent design that make
a specific stent more or less suitable for a particular type
of lesion or anatomy: the "average" coronary lesion,
the lesion situated on a curve, the ostial lesion, the bifurcational
lesion, the lesion located at the left main stem, the calcified
lesion, the chronic total occlusion, the small vessel, the saphenous
vein graft, acute or threatened vessel closure, and special
situations such as coronary aneurysms and perforations. (J Am
Coll Cardiol 2002;40:1021-33) Oc 2002 by the American College
of Cardiology Foundation
The implantation of coronary stents
is an integral part of most interventional procedures for percutaneous
revascularization. The wide acceptance of coronary stenting
was based on the results of the Belgian Netherlands STENT (BENESTENT)
(1) and the STent REStenosis Study (STRESS) (2) trials and was
facilitated by the elimination of anticoagulant therapy after
stent implantation .
The growing use of stents has stimulated
the introduction of a number of different stent designs. Table
1 illustrates the characteristics of most of the stents
available in 2002. The rapid increase in the number of designs
makes any list quickly outdated. Some stent designs are similar,
whereas others differ significantly. There are many reasons
why different designs have been proposed. Besides the legal
requirement to overcome a specific patent, there are concepts
of physiologic mechanisms that stimulated inventors to introduce
new designs. A primary concern of stent development was the
need to increase flexibility to facilitate safe delivery. Manufacturers
try to achieve this goal without compromising radial support
and lesion coverage. Another element important for optimizing
the clinical utility of a stent is its radiologic visibility.
Many of the engineering considerations in stent design were
adopted to improve the global acceptability of the device, rather
than making a stent design for a specific type of coronary lesion.
In clinical practice, the operator must decide which stent is
most appropriate for the patient. This article focuses on the
features of stent design that make a specific stent more or
less suitable for a particular type of lesion or anatomy.
Types of stents.
Stents can be classified according to their
mechanism of expansion (self-expanding or balloonexpandable),
their composition (stainless steel, cobalt-based alloy, tantalum,
nitinol, inert coating, active coating, or biodegradable), and
their design (mesh structure, coil, slotted tube, ring, multi-design,
or custom design) ( Table1
). According to the manufacturers, all stents are suitable for
implantation in native coronary arteries of the appropriate
size. Some stents are approved for implantation in vein grafts.
Few stents are specifically designed to be implanted in a particular
lesion. The absolute or relative contraindications to the use
of stents apply to stents in general and not to a specific stent.
Possible exceptions are the Multilink Ultra Stent (Guidant,
Temecula, California), which is designed for vein graft implantation
with a nine-cell design, by contrast with the six-cell design
of the Multilink Tetra. The JoMed polytetrafluoroethylene (PTFE)-covered
stent (JoMed, Rangendingen, Germany) is specifically made for
uncommon applications such as coronary ruptures, aneurysms,
and degenerated saphenous vein grafts.
Different characteristics such as strut thickness, metal to
artery ratio, degree of radiopacity, degree of foreshortening,
and recoil of many currently used stents are shown in Table
1. All stents are now available premounted on a dedicated
delivery system. The capacity of a stent to span a lesion depends
not only on the diameter of the crimped stent (Table 2), but
also on the amount of friction of the delivery system and stent,
flaring of the distal struts during interaction with the lesion,
flexibility of the stent and of the delivery balloon, and pushability
of the delivery system. It is not surprising to observe a stent
with a larger crossing profile cross a lesion easier than a
narrower stent with less flexibility.
Two interesting findings came from the stent versus stent randomized
trials: 1) the GR-II stent (Cook, Bloomington, Indiana) proved
clearly inferior-as far as early complications, binary restenosis,
and target lesion revascularization rate-to the Palmaz-Schatz
stent (Cordis, a Johnson & Johnson Company, Warren, New
Jersey) (6); and
2) the performance of the various other stents and the associated
clinical outcome were not different from the Palmaz-Schatz stent.
The slightly better deliverability of some stents compared with
the Palmaz-Schatz stent, as seen in some of equivalency trials,
has now only historical value. Stents used nowadays perform
significantly better than any of the early-generation devices.
Abbreviations and Acronyms
IVUS = intravascular ultrasound
PTFE = polytetrafluoroethylene
PTCA = percutaneous transluminal coronary angioplasty
Based on our experience with multiple stent systems, we submit
the following observations concerning the application of different
stents for specific lesion subsets.
The "average" coronary lesion.
Stents were initially indicated for proximal,
non-angulated lesions, whereas subsequent generation stents
were developed for lesions of tortuous anatomy and complex situations.
Some stents are more flexible than others or have a smaller
profile and therefore are more deliverable. These extra features
become necessary only in selected situations. Most stents currently
available are suitable for the majority of coronary lesions,
with some exceptions.
The stents to be used in the "average" coronary lesion
are the new slotted, tubular stents and some new designs of
ring stents.
The primary goal for stenting most coronary lesions is to achieve
the optimal lumen cross-sectional area without traumatizing
the artery. Currently, the achievement of a large final lumen
diameter is the most secure means of limiting restenosis . Other
appropriate concerns for stent choice are adequate lesion coverage,
minimal recoil, and limited plaque prolapse. In addition, because
stent length is an independent predictor of restenosis, it is
preferable to avoid the use of excessive metal
.
The Palmaz-Schatz stent led the way but now has passed the baton
to the BxVelocity (Cordis), as demonstrated in the Very Early
Nimopidine Use in Stroke (VENUS) trial, a multicenter registry
of the Cordis BxVelocity stent (10). It is likely that the BxVelocity
stent will be replaced by the sirolimus-coated BxVelocity (11,
12). The BxVelocity stent is applicable for everyday use, and
there are only a few conditions in which this stent may not
be satisfactory. The BxVelocity stent is available in three
different patterns of cells according to the vessel size in
which the stent will be implanted: six cells for vessels up
to 3 mm, seven cells for vessels up to 4 mm, and nine cells
for vessels up to 5 mm. The new version, BxSonic (Cordis), has
the same stent mounted on an improved delivery system that is
compatible with the 5F guiding catheter (lower profile proximal
hypotube shaft, 1.9F vs. 2.6F shaft of the BxVelocity, and 0.5-mm
balloon overhang on each side).
The heparin-coated Palmaz-Schatz stent had a low incidence of
subacute stent thrombosis, with only five thrombotic events
(0.4%) in 1,169 patients treated with this stent in the following
trials: the BENESTENT II pilot study , BENESTENT II randomized
study , and the Total Occlusion Study of CAnada (TOSCA) , as
well as in two protocols involving patients with acute myocardial
infarction: the stenting in Primary Angioplasty in Myocardial
Infarction (PAMI) pilot study and the stent PAMI randomized
study . A multicenter feasibility study (use of the Hepacoat
BxVelocity stent and an antithrOmbotic regimen of asPirin alonE
[HOPE]) is under way to examine the safety of the heparin-coated
BxVelocity stent (Hepacoat, Cordis) in "low-risk"
patients treated with antiplatelet therapy consisting of only
aspirin. The initial results in 202 patients showed no acute
stent thrombosis and a rate of 1% of subacute thrombosis (one
patient with thrombocytosis and one with post-trauma).]
The Multilink Tetra stent (Guidant) has functional characteristics
that are similar to the BxVelocity stent. The overall performance
of these two stents is excellent, with only selected situations
where the Tetra appears to be more deliverable. A unique feature
of the Tetra delivery system (similar to the Ultra) is its shaft
length of 143 cm, which is 3 cm longer than the BxVelocity stent,
whereas all the other delivery systems are 138 or 135 cm long.
Compared with the Multilink Tetra stent, the Multilink Penta
stent (Guidant) has a modified link pattern, which improves
flexibility and scaffolding and maintains side-branch access
with the possibility to expand the cell toward the side branch
up to 4 mm in diameter.
The careful observer may find more stent-to-vessel conformability
with the Tetra stent, but no one knows whether this feature
has any clinical consequences. Preserving the original shear
stress pattern of the arterial segment may lower the amount
of tissue hyperplasia .
The NIR stent (Medinol, Jerusalem, Israel; and Scimed, Boston
Scientific, Maple Grove, Minnesota), with its new "sox"
delivery system, is another important stent to be considered
for the "average" lesion. The NIR stent provides excellent
plaque coverage, which may be an advantage in lesions prone
to plaque prolapse. Plaque may prolapse between stent struts
in large vessels with a reference diameter ?4 mm. The NIR stent
is available with a seven-cell or nine-cell structure, which
improves plaque support in large vessels, including saphenous
vein grafts. The sox delivery system protects the stent while
negotiating through calcified lesion or crossing another stent.
These features are unique to this type of stent delivery system.
The performance of this stent was evaluated against the Palmaz-Schatz
stent in the NIR Vascular Advanced North American (NIRVANA)
trial randomized study (20). This trial reported a follow-up
restenosis rate of 19.3% for the NIR stent and 22.4% for the
Palmaz-Schatz stent. The moderate rigidity of the NIR stent
discourages its use through tortuous segments and for lesions
located at a severe bend. Because the NIR stent becomes rigid
on deployment, this stent may produce a hinge effect that is
associated with an increase in restenosis . Figure 1 demonstrates
the hinge effect caused by the NIR stent. This lesion restenosed
four months later at the distal extremity of the stent (Fig.
2). The operator should foresee this possibility and select
a more flexible type of stent in lesions with a small radius
of curvature
The positive features of these three stents are also related
to the delivery balloon:
1) there is now near perfect retention,
which has eliminated the problem of stent loss;
2) there is
minimal overhang of the delivery balloon from the stent, which
limits trauma and the risk of peri-stent dissection; and
3)
there is low compliance, which assures a more homogeneous stent
deployment (Fig. 3).
The beStent (Medtronic AVE, Minneapolis, Minnesota) and now
the beStent 2, with a closer strut design, are other stents
to consider. The unique feature of this stent is the presence
of proximal and distal gold markers that allow very precise
placement. Another positive feature of the beStent, but not
the beStent 2, is the presence of a large or open cell design
that facilitates access to side branches.
The Biodivysio stent (Biocompatibles, Galway, Ireland) is another
sturdy device with optimal scaffolding that can be considered
for most lesions. This stent is available also with an open-cell
design that is suitable for lesions involving the origin of
side branches. Compared with the open-cell design, the added
support design has an extra strut between interlocking arrowheads,
which provides greater coverage for lesions that require additional
support.
The Biodivysio stent was recently evaluated against the Duet
stent (Guidant) in a randomized trial (bioDlvysio STent IN randomized
Control Trial [DISTINCT]). Both stents showed an excellent low
restenosis rate of 19% in selected favorable lesions. The standard
Biodivysio stent delivery system appears to be more rigid compared
with other stents and is not ideal for very tortuous arteries.
New versions of the delivery system will soon be released to
overcome this potential limitation. The availability of a small-vessel
design with this stent, which is very trackable and has a low
profile, should be kept in mind when confronted with complex
anatomy. A unique feature of the Biodivysio family is their
phosphorylcholine coating, which lowers platelet adhesion to
the stent struts and may be used as a platform for drug delivery.
Among the ring stents, the new S7 (Medtronic AVE) provides more
plaque coverage than the S670 and has an angiographic appearance
very similar to the slotted, tubular stents. This stent is appropriate
for most lesions. In addition, the flexibility, conformability,
and lower friction typical of the S7 ring design improves deliverability
in complex anatomies or when passing through a stent. An important
characteristic of the AVE delivery system is minimal balloon
overhang (Fig. 3).
Among the stainless-steel stents with a good track record, the
family of stents from PURR (Devon Medical, Hamburg, Germany)
and the V-Flex plus (Cook) should be mentioned.
To make the choice more difficult, the interventionist is confronted
with other excellent stents such as the Sorin Sirius Carbostent
(Sorin Biomedica Cardio, Saluggia, Italy), with its recently
refined delivery system (Sorin Syncro Carbostent). This stent
performs quite well in difficult anatomies and lesions, has
platinum end markers, and is covered with a thin layer of turbostratic
carbon with the intent to decrease its interaction with platelets.
A recent registry report showing a restenosis rate of 11% and
a bimodal distribution of the loss index (22) raises the possibility
of enhanced biocompatibility of the carboncoated stent for subjects
with an allergy to metal components present in stainless steel
(23). At least four other carbon-coated stents are currently
available in Europe: the BioDiamond (Plasma Chem, Mainz, Germany),
the Diamond Flex (Phytis, Dreieich, Germany), the MAC carbon
stent (AMG, Raesfeld-Erle, Germany), and the Tenax (Biotronik,
Berlin, Germany). Randomized trials are in progress to test
the hypothesis that these inertly coated stents may have advantages
over the stainless-steel stents.
Lesions situated on a curve (?90°) or immediately
followed by a curve.
Changing the natural conformation of a coronary
vessel may have an unfavorable effect on flow dynamics and increase
the risk of adverse events during follow-up (24).
For this reason, we prefer stents that conform to the longitudinal
profile of the vessel without producing plaque prolapse in the
curved segment. The traditional ring design, such as the S670,
is quite conformable but may allow too much plaque protrusion
when opened in a curved segment. In this respect, the new S7
is a significant improvement. Slotted, tubular stents with thin
struts are also conformable (PURA AS and AL 0.07, 0.075-mm beStent,
0.075-mm Sorin Carbostent, 0.08-mm Tenax, 0.09-mm Biodivysio,
and 0.09-mm JoStent). Strut thickness is not the only variable
that may affect conformability; the complete stent design may
be more important. For example, the NIR stent, which is thinner
(0.1 mm) than the BxVelocity (0.14 mm), has lower conformability.
The Tetra and Penta stents have variable strut thicknesses (0.091-0.124
mm), with excellent conformability. The NIRflex, the new version
of the NIR stent, also has excellent conformability.
Ostial lesions.
Ostial lesions are classified as either aortoostial
or coronary-ostial. For aorto-ostial lesions, the slotted-tube
design, preferably with strong radial support, low recoil, and
radiologic visibility, is the most appropriate one (25). New
ring designs such as the S670 and S7 are also appropriate in
this setting.
The recent availability of stents with end markers may improve
precise positioning. These stents have thin struts, so our preference
is to implant them only in coronary-ostial rather than aorto-ostial
locations. The strong elastic recoil inherent to the aorta favors
the use of thicker struts to provide greater resistance when
dealing with lesions involving the true coronary ostia or the
aortic insertion of a saphenous vein graft.
When considering the gold-plated NIR Royal for an aorto-ostial
lesion, the operator must balance its advantage of better visibility
and more precise positioning with its disadvantage of having
a higher angiographic restenosis rate
than the stainless-steel NIR (37.5% vs. 20.6%, p < 0.001),
as reported in the NIR Ultimate Gold-Gilded Equivalency Trial
(NUGGET) . Similar findings were reported with a gold-coated
stent manufactured by a different company .
For aorto-ostial lesions with a reference vessel size of ?4
mm in diameter, we have had a positive clinical experience with
the BxVelocity, the nine-cell NIR, and the Ultra. All of these
slotted-tube stents maintain good radial force, even when dilated
to large diameters.
Table 1. Stent Engineering Data
Bifurcational lesions.
When approaching a bifurcational lesion, it
may be preferable to have a stent with large side openings between
the struts that can easily permit passage of a balloon or second
stent into the side branch. Figure 4 shows several slotted-tube
stents with the cross-sectional area of the cell following stent
dilation and with the cross-sectional area of the same cell
following the maximal opening of a balloon inflated across the
cell into the side branch . Many slotted-tube stents are suitable
for stenting a bifurcation, with the exception of the NIR stent.
The closed-cell design of the NIR does not allow significant
expansion of the opening toward the side branch, even after
crossing and inflating a balloon. If the operator decides to
use the NIR stent, the seven-cell design should be used instead
of the nine-cell design.
Another option is to use a stent with a large side opening,
such as the Biodivysio open-cell design or the S670. The advantage
of this decision is that the initial access to the side branch
is facilitated. A possible disadvantage is incomplete prolapse
of one strut toward the side branch following a "kissing"
balloon dilation (i.e., dilating 2 balloons simultaneously into
both branches of a bifurcation). The concept of strut prolapse
from the main branch toward the side branch has been pioneered
by Dr. Marie Claude Morice and Dr. Tierry Lefevre and termed
"stenting both branches with one stent." When the
design is very open, there is less possibility for a strut to
straddle across the side branch. Slotted-tube stents that best
demonstrate this feature are the beStent and Carbostent, but
the BxVelocity and Tetra are also adequate (Fig. 5).
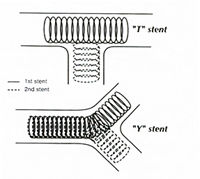
Whichever stent the operator uses for a bifurcation, it is important
to perform a "kissing" balloon inflation at the end
of the procedure to correct the stent distortion that occurs
after balloon inflation in the side branch (29). If the operator
finds it appropriate to stent both branches, we recommend the
modified T or V techniques. Lesions located at the left main
stem. Left main stem lesions may involve treatment of an aorto-ostial
lesion and/or a lesion located in the body of the left main
artery. Occasionally, there is a need to treat the distal left
main stem as a bifurcational lesion.
The reference size of the left main coronary artery is favorable
to stent implantation in terms of the restenosis rate. The major
problem is that in an unprotected left main artery, stent restenosis
may manifest either as sudden death or unstable angina rapidly
followed by death. For this reason, when stent implantation
in an unprotected left main artery is clinically indicated,
we frequently debulk the lesion with directional atherectomy
to minimize the risk of restenosis (30).
Selection of the stent to be used depends on the issues discussed
previously concerning ostial lesions and bifurcational lesions.
The only unique aspect of left main stenting is the final size
of this vessel. It is not unusual, especially if intravascular
ultrasound (IVUS) is employed (31), to perform a post-stent
dilation with a balloon >4 mm. For this reason, when the
left main artery appears large, we recommend using slotted-tube
stents that can be expanded >4 mm. The NIR nine-cell, BxVelocity,
Tetra and Ultra are excellent choices. When the stent is overexpanded
and it is located in the aorto-ostial position, it is important
to realize that a significant foreshortening will occur. The
operator should take this into account when initially placing
the stent by placing the proximal end of the stent 1 to 2 mm
into the aorta. In addition, if the ostium is left uncovered,
the operator should not hesitate to place a second stent. The
use of IVUS may be beneficial in determining the precise position
of a stent. The use of stents with no foreshortening and with
markers like the beStent or Carbostent is an important consideration
in this context. As a general rule, when treating an aorto-ostial
lesion, it is important to avoid using a stent that is very
short, such as an 8- or 9-mm stent. This recommendation becomes
even more important when dealing with a lesion at the ostium
of the left main artery. We have seen stents ejected from the
left main stem at the time of postdilation due to their short
anchoring length.
Calcified lesions.
Despite the widespread notion that
calcium affects stent expansion , there are only a few reports
specifically dealing with this issue . The general view is that
stent expansion in a calcified lesion will yield a smaller final
lumen than will expansion in a noncalcified lesion. Adequate
final expansion is usually achieved by stretching the non-calcified
arc of the vessel. If an adequate final lumen size is achieved,
this approach does not seem to affect restenosis. To obtain
an adequate final lumen size, it is important to have a slotted-tube
stent with minimal recoil and good radial strength. The NIR,
BxVelocity, Tetra, and AVE-S family stents are all reasonable
choices.
In calcified lesions, the most important part of the procedure
is adequate preparation of the lesion before stent implantation.
The amount of calcium visible on X-ray underestimates the amount
of calcium observed on IVUS. Intravascular ultrasound can also
distinguish whether the calcium is in a superficial or deep
location . Efforts to evaluate the lesion and to prepare the
implantation site with rotational atherectomy or by cutting
the balloon will be well rewarded. Post-dilation with a short,
non-compliant balloon is another important step.
Chronic total occlusions.
Stent implantation for chronic total occlusions
must address two problems: 1) the amount of plaque mass in these
types of lesions is large; and 2) it is not rare that passage
through the occluded segment occurs by creating a false lumen
with reentry.
These two elements mandate the insertion of a stent with good
lesion coverage and radial support. The PalmazSchatz stent was
used in the Stenting In Chronic Coronary Occlusion (SICCO) study
(36), which reported a significant benefit of stent implantation
(32% restenosis) in comparison with percutaneous transluminal
coronary angioplasty (PTCA) (74% restenosis) after recanalization
of chronic total occlusions. In TOSCA (15), 410 patients with
nonacute native coronary occlusions were randomized to PTCA
or primary stenting with the heparin-coated Palmaz-Schatz stent.
With 95.6% angiographic follow-up, primary stenting resulted
in a 44% reduction in failed patency (10.9% vs. 19.5%, p = 0.024)
and a 45% reduction in clinically driven target vessel revascularization
at six months (8.4% vs. 15.4%, p = 0.03).
In addition to various slotted-tube stents (e.g., NIR, BxVelocity),
the Wallstent needs to be considered for dealing with a large
vessel, especially for the right coronary artery .
The general rule for treating a chronic total occlusion is to
use a stent with good plaque coverage with a closed-cell design,
allowing minimal plaque prolapse in this setting where there
is a large plaque burden.
Figure 4. Area of the stent cell at nominal
(solid bars) and maximal (open bars) expansion for several slotted-tube
stents.
Vessels smaller than 3.0 mm in diameter.
Stent implantation in small vessels is associated
with a number of problems. Initially, no stents were specifically
made to be expanded in small vessels with the capacity to gain
optimal radial support at diameters between 2.5 and 3.0 mm.
Only recently have stents become available such as the Mini
Crown, beStent (4 crowns), Biodivysio SV (small vessels), six-cell
BxVelocity, Multilink Pixel, 2.5-mm Carbostent four-cell, and
small-vessel Pura Vario AS, which are designed to fit vessels
<3 mm. The most important attributes of these stents are
their improved flexibility, capacity to reach distal lesions,
and very thin strut structure.
The recent introduction of stents specifically designed for
small vessels has allowed the performance of randomized trials
without interference from the implantation of stents not dedicated
to small vessels. Figure 6 summarizes the results of four recently
completed studies (38-41). In three of them, the beStent-4 crown
(Medtronic AVE) was used;
A
B
C
D
Figure 5. Examples of stent strut prolapse from the main branch
toward the side branch after "kissing" balloon inflation
(arrows). (A) The Sorin Sirius Carbostent (Sorin Biomedica Cardio,
Saluggia, Italy). (B) The beStent 2 (Medtronic AVE, Minneapolis,
Minnesota). (C) The BxVelocity (Cordis, a Johnson &Johnson
Company, Warren, New Jersey). (D) The Multilink Tetra stent
(Guidant, Temecula, California).
Figure 1. (A) Baseline angiogram of a lesion (arrow) in the
proximal right coronary artery. (B) Angiogram after implantation
of a nine-cell, 16-mm-long NIR stent. The hinge site at the
end of the stent is clear(arrow).
Crossing Profile
Crossing Profile*
Product Manufacturer 2.5-mm Diameter 3.0-mm Diameter
AVE S670 Medtronic 1.09
AVE S660 Medtronic 0.99
beStent 2 Medtronic 1.07 1.17
Biodivysio AS Biocompatibles 1.07
Biodiwsio SV Biocompatibles 0.84
BxVelocity Cordis, Johnson &Johnson 1.07 1.17
BxSonic Cordis, Johnson &Johnson 1.07 1.14
Carbostent Sorin 1.02 1.04
Multilink Tetra Guidant ACS 1.04 1.12
Multilink Penta Guidant ACS 1.04 1.07
Multilink Pixel Guidant ACS 0.93
NIR with sox Medinol, Boston Scientific 1.09 1.12
Express Boston Scientific 1.02 1.09
*Data presented reflect measurements performed by individual
manufacturers; the method used to measure and the exact site
of measurements may differ among different stents.
1 September 18, 2002:1021-33
Figure 2. Four-month follow-up angiogram of the lesion in Figure
1, showing restenosis at the hinge site (arrow).
p< 0.001
I
p= 0.36
p= 0.04 p= 0.74
60
50 -
47%
PTC A
PTCA
PTC A
PTCA
beSMART n=381
SISA n=351
RAP ISAR-SMART
n=426 n=404
Figure 6. Restenosis rates in randomized trials of small-vessel
stenting versus balloon PTCA. beSMART = BEstent in SMal ARTeries;
SISA = Stenting In Small Arteries; RAP = Restenosis en Arterias
Pequenas; ISAR-SMART = Intracoronary Stenting or Angioplasty
for Restenosis reduction in Shall ARTeries; PTCA = percutaneous
transluminal coronary angioplasty.
Continued: Vessels smaller than 3.00mm in diameter.
in the other study, the Multilink was initially implanted and
then substituted by the Duet (Guidant). In two studies, the
results showed a superiority of stenting over PTCA, and in the
other two studies, the restenosis rates were equivalent.
An interesting observation came from the Intracoronary Stenting
and Angiographic Results: Strut Thickness Effect on REstenosis
Outcome (ISAR-STEREO) study (42). The authors reported a significantly
lower restenosis rate in vessels larger than 2.8 mm (15.0% vs.
25.8%, p < 0.003) after implantation of the thin-strut (0.05
mm) Multilink stent, compared with the thicker strut (0.14 mm)
Duet stent. Whether this finding also applies to small vessels
needs to be evaluated.
To ensure more flexibility and easier delivery
to lesions located in small vessels, we use dedicated small-vessel
stents with thin struts. The Biodivysio SV and beStent (4 crowns)
stents are probably the most suitable stents to be implanted
on lesions located in small vessels. The stent delivery system
of these stents is about 0.75 mm in profile, making them the
smallest profile stent delivery system. The Sorin Carbostent
is another thin-strut stent available in a small vessel size.
All of these stents, with the exception of the Biodivysio SV
stent, are visible under X-ray thanks to distal and proximal
radiopaque markers.
The BxVelocity, with the dedicated six-cell stent, and the Multilink
Pixel, a new, small-vessel stent by Guidant, are also good choices.
In comparison to the other small-vessel stents, these two stents
do not have thin struts and are visible under X-ray.
Saphenous vein grafts.
Implanting stents in lesions located
in a saphenous vein graft usually involves dealing with a lesion
located in a large vessel. Because a major goal is to minimize
trauma to the plaque and give maximal lesion coverage to avoid
the risk of distal embolization, selfexpandable stents are very
useful in this setting. The Wallstent or nitinol NIR stent is
suitable, especially for long lesions in these locations.
One persisting problem with stent implantation
in vein grafts is that future events may result from progression
of other lesions that were not considered critical at the time
of initial stent implantation in the target lesion (43). This
issue will be evaluated by prospective studies comparing a strategy
of focal stent implantation in the critical lesions with a strategy
aimed at implanting stents also in lesions that are not angiographically
critical.
Vein graft stent implantation must be performed
with a stent that provides optimal lesion coverage and is available
in different lengths (vein grafts require longer stents).
Other suitable stents for operators who prefer balloonexpandable
stents are the Ultra version of the Multilink design specifically
made for vein graft lesions (Guidant) and the nine-cell NIR
stent.
The most important issue concerning stenting
of vein grafts is the risk of distal embolization. Our experience
is that no particular currently available stent is more likely
than another to limit these complications. The recent introduction
of a protective balloon on a wire system (in the Saphenous vein
graft Angioplasty Free of Emboli [SAFE] [44,45] and the Saphenous
vein graft Angioplasty Free of Emboli Randomized [SAFER] [46]
studies) and a number of filter devices has improved the safety
of vein graft interventions.
A discussion of vein graft stenting would not be complete without
mentioning the PTFE-covered stent. This device has the potential
to entrap the friable plaque present in vein grafts, with a
positive impact on distal embolization and late restenosis (47,48).
A similar device, with the covering membrane made of bovine
pericardium, is currently under clinical evaluation (Fig. 7).
Figure 7. A stent with the covering membrane made of bovine
pericardium.
Early and threatened closure.
Stents were initially developed to treat acute
closure from balloon dilation (49,50). The stents used most
extensively were the GianturcoRoubin I stent (51,52) and the
Palmaz-Schatz stent . Higher rates of success, even in lesions
of complex anatomy and long dissections, were reported with
the GianturcoRoubin II stent and with the AVE II MicroStent.
The ideal stent for treating a dissection with impending closure
should have an easy and predictable delivery, even without an
optimal guiding catheter or guidewire support. We have nicknamed
this condition "the panic stent." The Pixel, the Sonic,
and the S660 are some of the most deliverable stents in complex
anatomies.
Treatment of dissections may require placing a short stent distal
to an already deployed stent, usually to treat a residual distal
dissection not evident at the time of the first stent implantation.
An incompletely sealed dissection, especially in the setting
of impending closure, remains one important predictor of stent
occlusion, even with the use of highpressure dilation after
stent implantation and with administration of aspirin and ticlopidine
(55). Therefore, a stent with a predictable delivery and with
which the operator feels confidence, is likely to be the preferred
one. It will also result in a low incidence of stent thrombosis
if it provides good coverage of the dissection without plaque
prolapse.
Special situations.
There are instances in which the operator
needs to creatively modify the tools available to provide a
new device capable of satisfying an unusual condition. Three
of these situations are the treatment of severe focal aneurysmal
dilation of a coronary artery, diffuse aneurysmal disease of
vein grafts, and, occasionally, coronary perforations. The use
of an autologous vein graft-coated stent is an interesting solution
pioneered by Stefanadis et al. (56,57). The Tetra, BxVelocity,
NIR, and other slotted-tube stents are good platforms on which
the autologous vein can be mounted.
Coronary perforations are rare but need a rapid and effective
treatment. The new PTFE-covered stent is now available in a
premounted form and is probably the best
device to treat a coronary perforation or a coronary aneurysm
.
Another use for this covered stent is the treatment of aorto-ostial
coronary and ostial saphenous vein graft lesions. Because of
the high incidence of repeat restenosis in aorto-ostial lesions,
the PTFE-covered stent should be considered among the options,
even at the time of the first percutaneous procedure.
Drug-eluting stents.
The goal of maximizing lumen gain with mechanical
scaffolding to prevent acute and chronic recoil and to seal
any dissection, coupled with the possibility to eliminate excessive
tissue proliferation, gave birth to drug-eluting stents. As
of early 2002, all drug-eluting stents are still investigational
devices. Soon, some of them will become available for clinical
use in Europe and outside the U.S.
Drug-eluting stents can be classified according to the specific
stent design, presence or absence of a polymer to absorb the
drug, type of polymer, type of drug, and release pattern.
Currently, the V-Flex Plus coronary stent (Cook) and the Achieve
coronary stent system (manufactured by Cook and distributed
by Guidant) are used to deliver paclitaxel adhered to the stent
surface with no polymer. The JoMed coronary stent graft and
the JoMed Flex (nanoporous ceramic coating) are also used with
no polymer to deliver tacrolimus.
Stents that employ a polymer carrier for local drug delivery
are the BxVelocity (Cordis) for sirolimus; the NIR Conformer
(Medinol and Scimed) and the Express (Boston Scientific) for
paclitaxel; the Biodivysio Matrix LO (Biocompatibles) for dexamethasone,
prednisolone, batimastat, estrogen, and angiopeptin; the Tetra
(Guidant) for actinomycin D; the AVE S7 (Medtronic AVE) for
c-rnyc antisense (resten-NG); and the Tsunami (Terumo Co., Tokyo,
Japan) for statins. All of the aforementioned drug-eluting stents
are in clinical trials with different degree of progress, with
the exception of resten-NG, which has not yet been evaluated
in humans. Recently, the actinomycin D and batimastat programs
have been discontinued because of a lack of efficacy.
The drug-eluting stent programs under more advanced clinical
evaluation are the Cypher (sirolimus) and Taxus (paclitaxel).
The most important achievements of the Cypher program are: 1)
a 0% rate of six-month angiographic restenosis in the RAndomized
study with the sirolimus-eluting Bx VELocity balloon-expandable
stent in the treatment of patients with de novo native coronary
artery lesions (RAVEL) trial and sustained clinical efficacy
at one-year follow-up (61); 2) persistent good vessel patency
at two-year follow-up in the First-In-Man study (62); 3) a low
30-day event rate in the U.S. multicenter, randomized, double-blind
study of SIRolImUS-eluting stent in coronary lesions (SIRIUS)
trial (63); 4) completion of a pilot in-stent restenosis study
(64); 5) bifurcational and small vessels with long lesions (European
SIRIUS [E-SIRIUS]), projects with enrollment recently completed;
6) a left main stem registry and the Arterial Revascularization
Therapy Study (ARTS) II registry, close to initiation; and 7)
the first drug-eluting stent in the market for coronary applications
(expected for April 2002).
The most important achievements of the Taxus program are: 1)
a 0% rate of six-month angiographic restenosis in the pilot
Taxus I trial ; 2) completion of enrollment and a low early
event rate in Taxus II; and 3) acceptable incidence of six-month
major adverse cardiac events (17%, consisting mainly of late
target vessel revascularization) in the Taxus III registry for
treatment of in-stent restenosis .
Table 3. Stent Consumer's Guide
Product Manufacturer Deliverability Scaffolding Side-Branch
Access Accurate
Positioning Large
Vessels Small
Vessels
AVE S670 Medtronic ++++ +++ ++
AVE S7 Medtronic ++++ +++ +++
Biodivysio Biocompatibles ++ ++ ++
BxVelocity/Sonic Cordis, Johnson &Johnson +++ ++ ++
JoStent graft Jomed ++++ NA +++ 0
Multilink Penta Guidant +++ +++ ++ +++
NIR, 7 cells and 9 cells Medinol, Boston Scientific ++++ +++
NIR Royal Medinol, Boston Scientific ++++
Express Boston Scientific +++ ++ +++
AVE S660 Medtronic AVE +++ ++ NA
Biodivysio SV Biocompatibles +++ +++ NA ++
Multilink Pixel Guidant ACS +++ +++ ++ NA ++
++++ = excellent; +++ = very good; + + = good; + = acceptable;
0 = unsuitable; NA = not applicable.
Figure 8. Drug delivery to the vessel wall with various stent
designs. The color chart corresponds to the amount of drug concentration.
Table 3. Stent Consumer's Guide
Product Manufacturer Deliverability Scaffolding Side-Branch
Access Accurate
Positioning Large
Vessels Small
Vessels
AVE S670 Medtronic ++++ +++ ++
AVE S7 Medtronic ++++ +++ +++
Biodivysio Biocompatibles ++ ++ ++
BxVelocity/Sonic Cordis, Johnson &Johnson +++ ++ ++
JoStent graft Jomed ++++ NA +++ 0
Multilink Penta Guidant +++ +++ ++ +++
NIR, 7 cells and 9 cells Medinol, Boston Scientific ++++ +++
NIR Royal Medinol, Boston Scientific ++++
Express Boston Scientific +++ ++ +++
AVE S660 Medtronic AVE +++ ++ NA
Biodivysio SV Biocompatibles +++ +++ NA ++
Multilink Pixel Guidant ACS +++ +++ ++ NA ++
++++ = excellent; +++ = very good; + + = good; + = acceptable;
0 = unsuitable; NA = not applicable.
In the evolution of these special scents, we will also see
new stent designs made to maximize uniform drug delivery to
the vessel wall (Fig. 8).
Conclusions.
Despite all of the theoretic and practical
considerations provided for selecting a particular stent to
treat a specific lesion, the individual experience and confidence
of the operator are paramount. No rationale for choosing a specific
stent for a specific lesion is yet supported by randomized trials.
Nonetheless, a large number of observational studies support
the views expressed in this report.
Except for the use of a stent to prevent threatened occlusion,
stents are implanted with the intent to prevent restenosis.
The operator should strive to reach this goal while maximizing
the patient's safety. Judicious stent selection, balloon sizing,
and lesion preparation to achieve an optimal final lumen dimension
remain the most important goals in percutaneous coronary interventions.
For those interested in seeing comparisons based on personal
experience, we propose our point of view in a "consumer's
guide" format (Table 3).
With the advent of drug-eluting stents, many of these considerations
and recommendations may be altered. In the era of almost zero
late loss, the concept of maximizing lumen gain at the time
of stent implantation may not be as important as it appears
today. The experience with drugeluting stents may change the
technique of stenting, but one goal that will not change and
will become even more important is the reliable delivery of
the stent to the lesion.
Examples of Guide Wires

Coronary Dilatation Catheter Examples
OTW%20coronary%20dilatation%20catheter.png)
OTW%20coronary%20dilatation%20cathetercompletion.png)