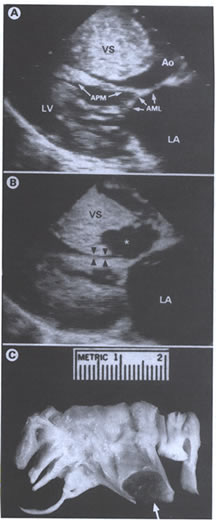
Figure 39m
Anomalous papillary muscle insertion
directty into anterior mitraL leaflet (AML) in patient with obstructive
HCM.
A. Before myotomy-myectomy:
parasternal Long-axis echocardiogram shows AML in direct continuity
with the hypertrophied anomalous anterolateral papillary muscle (APM),
which displaced anteriorly within the left ventricular cavity, producing
a long area of midcavity muscular contact with the ventricular septum
(VS) and outflow obstruction (arrows); tips of the mitral leaflets coapt
in the usual position, and typical systolic anterior motion is absent
(small arrows).
B. After myotomymyectomy: Long-axis echocardiogram shows extensive muscular
resection , extending from base of the septum to beyond the distal margins
of the anterior mitral leaflet; nevertheless, a Large area of direct
muscular contact remains after operation between papillary muscle and
ventricular septum (arrowheads), which is responsible for persistent
and marked obstruction to left ventricular outflow. C. Mitral valve
specimen excised at operation; a massively hypertrophied anterolateral
anomalous papillary muscle (arrow) inserted directly into the body of
the anterior leaflet. Ao = aorta; l.A = left atrial; LV = left ventricle.
(From Klues HG et al with permission of the authors ind ippincott William and Wilkins.)