


Standard 2D Ultrasound Examination of the Heart
It is possible to use fetal echocardiography
to identify congenital heart defects by identifying abnormalities
of the four-chamber view of the heart in fetuses with heart
defects. The standard basic cardiac examination includes a 4-chamber
view of the fetal heart. If technically feasible, an extended
basic cardiac examination can also be attempted to evaluate
both outflow tracts.
Four-Chamber View of the Heart
When the ultrasound beam is directed perpendicular to the chest of the fetus, four-chambers of the fetal heart are identified. These chambers consist of the right and left atrial and ventricular chambers, with their respective valves that connect the atrial with the ventricular chambers.The following images illustrate the ultrasound approach used to examine the four-chamber view.
These images and content below are mainly from Greggory R. Devore, M.D., author of Fetal Echocardiography at www.fetal.com and www.fetalecho.com
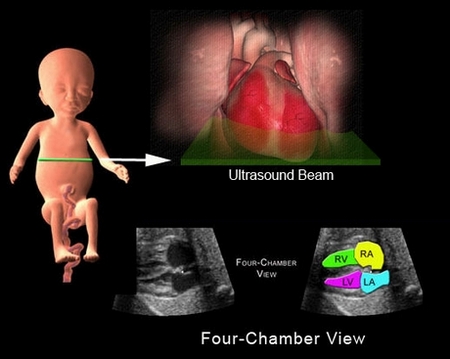
Imaging the four-chamber view is accomplished by directing the ultrasound beam perpendicular to the fetal chest. At this level, the four-chamber view is identified. This view contains the right atrium (RA), left atrium (LA), right ventricle (RV) and left ventricle (LV).
The below is the normal
four-chamber view of the fetal heart.
Normal 4-Chamber View (Video 1):
Please refer to the color picture above the video and to the right in interpreting the structures in this video, showing the right ventricle and atrium on the top, and the left ventricle and atrium (separated by the interventricular septum) on the bottom half of the video. To the left in the video are the apices of the right and left ventricles separated by the interventricular septum, while to the right are the right and left atria separated by the interatrial septum. The tricuspid valve can be seen opening and closing the right atrioventricular opening, while the mitral valve opens and closes the left atrioventricular opening.
Hypolastic Left Heart Syndrome (below):
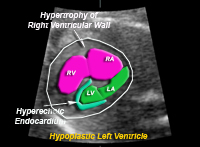
Labeled Image of the hypoplastic left ventricle. RV=right ventricle, LV=left ventricle, RA=right atrium, LA=left atrium
The illustration below is an example of an abnormal tricuspid valve of the right ventricle. The valve is displaced low in the right ventricular chamber. This results in changes in the four-chamber view that include a larger right atrium, smaller left atrium, and abnormal valve motion of the tricuspid valve.

Labeled Image of the hypoplastic left ventricle. RV=right ventricle, LV=left ventricle, RA=right atrium, LA=left atrium
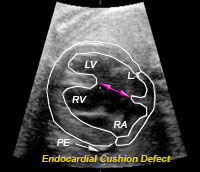
This is an endocardial cushion defect. The arrows demonstrate the absence of the ventricular and atrial septum. There is also fluid around the edge of the heart (PE) that should not be present. LV=left ventricle, LA=left atrium, RV=right ventricle, RA=right atrium
Limitations of the Four-Chamber View
Although the four-chamber view is useful for identifying abnormalities of the fetal heart, several defects may always demonstrate an abnormal four-chamber view. The reason for this is because heart defects may only involve the outflow tracts. The outflow tracts consist of the main pulmonary artery exiting the right ventricle and the aorta exiting the left ventricle. The reason that the four-chamber view does not identify these malformations is because the image of the four-chamber view is obtained at the level of the ventricles and atria, and not at the levels of the outflow tracts.
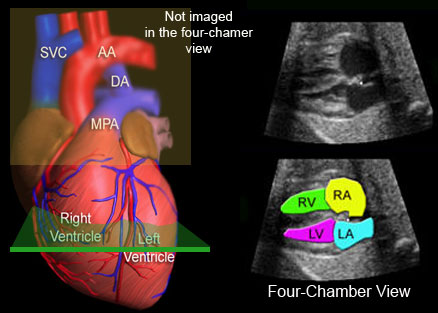
This illustrates the level that the four-chamber view is imaged (green). The main pulmonary artery (MPA), ductus arteriosus (DA), and the aorta (AA) are not imaged at the level of the four-chamber view. SVC=superior vena cava, RV=right ventricle, RA=right atrium, LV=left ventricle, LA=left atrium.
Examination of the Outflow Tracts
There are several approaches that the
examiner can use to identify the outflow tracts of the heart
that use the four-chamber view as the initial reference image.
Rotational Technique
This technique was first described by
Dr. DeVore in 1992. After imaging the four-chamber view, the
physician rotates and then rocks the transducer to image the
ascending aorta and the main pulmonary artery. This maneuver
identifies that (1) the main pulmonary artery and aorta are
perpendicular to each other as they exit their respective ventricles,
(2) these vessels are similar in size, and (3) the aortic and
pulmonary valves are normal, and (4) the aortic arch.
Movement of the transducer used
to acquire the views using the Rotational Technique.
The Rotation Technique.
Video10:
This video above shows the hand
of the technician rotating the transducer face down and turning
to the left in a circle on the mother's abdomen.
Sweep Technique
This technique was described by Yoo et
al and Yagel et al and involves sweeping the transducer beam
in a transverse plane from the level of the four-chamber view
towards the fetal neck. By doing so, the outflow tract vessels
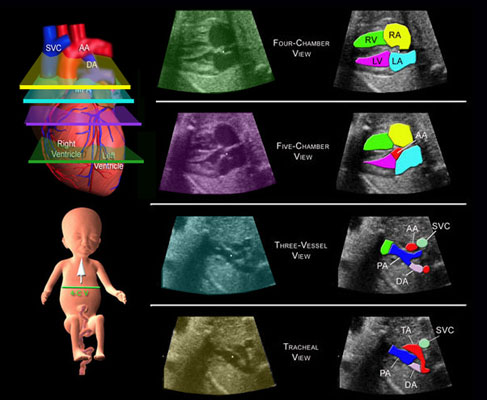
are observed. The sweep consists of the following views: four-chamber
view, five-chamber view, main pulmonary artery or 3-vessel view,
and the tracheal view (shown below in the video 11).
Video11: This illustrates movement of the transducer for obtaining the Sweep image sequences described above and seen below in Video 12.
Video12: Both ventricles and atria as well as the tricuspid and mitral valves are seen. The pulmonary artery is seen to open into the right ventricle, and the ascendiing aorta into the left ventricle.
The following images illustrate the four different levels used to identify cardiac anatomy using the Sweep Technique.
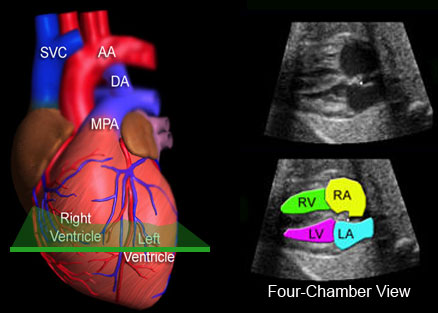
Four-Chamber View
This illustrates the level that the four-chamber view is imaged
(green). The main pulmonary artery (MPA) and the aorta (AA)
are not imaged at this level. SVC=superior vena cava, DA=ductus
arteriosus, RV=right ventricle, RA=right atrium, LV=left ventricle,
LA=left atrium.
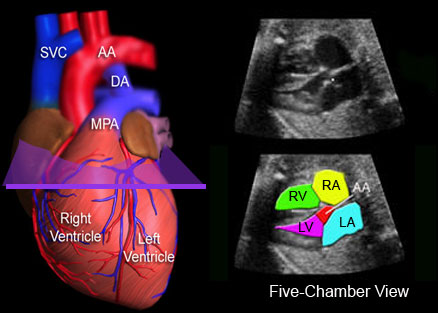
Five-Chamber View
This is the level of the five-chamber view and illustrates the
aorta (AA) exiting the left ventricle. RV=right ventricle, RA=right
atrium, LV=left ventricle, LA=left atrium.
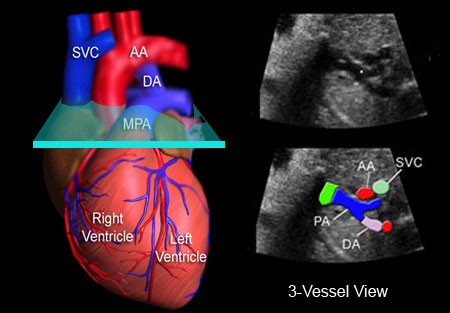
3-vessel View
This is the 3-vessel view because 3 vessels are observed; the
superior vena cava (SVC), the cross-section of the ascending
aorta (AA), and the full length of the main pulmonary artery
(PA). This is an important view because it illustrates the ascending
aorta perpendicular to the main pulmonary artery. If these two
vessels are not perpendicular to each other at this level, then
a serious heart defect, transposition of the great vessels,
is most likely present. DA=ductus arteriosus.
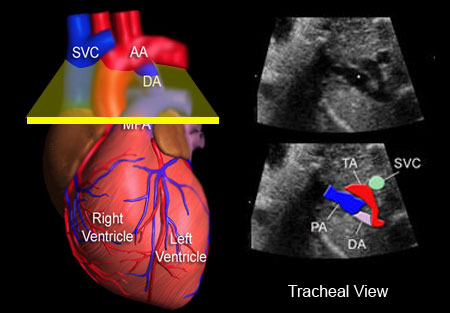
Tracheal View
This is the tracheal view because these vessels are at the level
of the trachea. This view is important because it illustrates
the transverse aortic arch (TA) and the ductus arteriosus (DA)
merging with the thoracic aorta.
Summary of All Views
The four-chamber view and the outflow tracts of the heart are
imaged by first locating the four-chamber view of the heart
and then sweeping the transducer towards the fetal neck. When
this is done, the five-bomber, 3-vessel, and tracheal views
are identified.
Examples of Pathology
The following are examples of heart abnormalities that are identified using the sweep technique.
This is an example of Transposition of
the Great Arteries. When this is present the left ventricle
gives rise to the pulmonary artery and the right ventricle to
the aorta. Because of fetal circulation this creates no problem
for the fetus. However, once birth occurs, the blood flow to
the lungs and body is abnormal. Newborns with this condition
require surgery to survive.
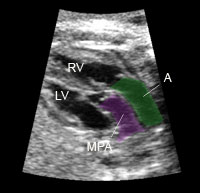
This illustrates the pathology. The aorta (A) exits the right ventricle (RV) and the main pulmonary artery (MPA) exits the left ventricle. This image is taken at the level of the 5-chamber view. Both the aorta and main pulmonary artery are parallel to each other instead of being perpendicular.
This is an example of Tetralogy of Fallot.
There is a ventricular septal defect that straddles the dilated
aorta. This defect is not usually seen in the four-chamber view.
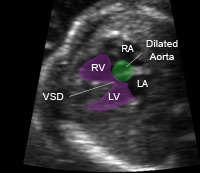
This illustrates the pathology. The aorta is increased in size and straddles the ventricular septal defect.
This is an example of an abnormal tricuspid valve of the right ventricle. The valve is displaced low in the right ventricular chamber. This results in changes in the four-chamber view that include a larger right atrium, smaller left atrium, and abnormal valve motion of the tricuspid valve. (Click on video 5 below)